Indeed, it seems that this is unlikely to be the case. Various surrogates for quantifying SLN tumor burden have been proposed, and in general, all correlate with disease outcomes. Microscopic tumor burden in sentinel lymph nodes predicts synchronous nonsentinel lymph node involvement in patients with melanoma. Nevertheless, many additional well-established prognostic factors are not incorporated into the staging system. Utjes D, Malmstedt J, Teras J, et al. 2017 (in press). The understanding of pathology of melanoma has evolved over the years, with the initial classifications based on the clinical and microscopic features to the current use of immunohistochemistry and genetic sequencing. Google Scholar. Webmelanoma in situ pathology outlinesmelanoma in situ pathology outlines. -, Cohn-Cedermark G, Rutqvist LE, Andersson R, et al. Similarly, a melanoma measuring 1.04mm thick would be recorded as 1.0mm in the pathology report and designated as T1b for staging. Dodds TJ, Lo S, Jackett L, Nieweg O, Thompson JF, Scolyer RA. Article Incorporation of additional prognostic parameters into computerized prognostic algorithms is likely to provide more individualized and accurate prognostic estimates [40]. the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in When assessing primary cutaneous melanomas, pathologists should provide a report with sufficient information to facilitate both accurate staging to occur and a reliable estimate of prognosis to be made. Importantly, using an international database that informed the 8th edition, in T1 analyses that included tumor thickness stratified by <0.8 mm versus 0.8 mm 1.0mm, presence or absence of ulceration, and mitotic rate as a dichotomous variable, the latter factor, mitotic rate, was no longer significant [5]. [10] Prior to 2009, there were no effective systemic drug therapies for patients with advanced melanoma which at that time had a 25% 1-year survival rate [6]. A combined pattern is characterized by an in situ or radially growing pattern combined with a nodular component. Mihm Jr MC, Clark Jr WH, From L . Melanoma in situ For several decades, the established benchmark for risk stratification for patients into prognostic groups has been the AJCC staging system. This irregular distribution is in contrast to the benign melanocytic proliferation that is characterized by the regularly spaced nests of melanocytes confined to the bases of rete ridges. 1991;126(4):438441. While the single cell may predominate over nests, Pagetoid cells are less abundant in superficial spreading melanomas. ISSN 1530-0285 (online) Nuclear chromatin is dense and nucleoli are often unapparent (Figure 8). 5). Distinguish mainly from dysplastic nevus and invasive melanoma of the skin: In suspected but not certain nevus or melanoma in situ, generally perform immunohistochemistry with SOX10, whereby melanocyte proliferation and nuclear pleomorphism is easier to see. The clinical diagnosis, classification and histogenetic concepts of the early stages of cutaneous malignant melanomas. Nature 2018;553:3474350. It is for this reason that both the T and N categories were combined to define the stage III groupings in the 8th edition (Table4). Wolchok JD, Chiarion-Sileni V, Gonzalez R, Rutkowski P, Grob JJ, Cowey CL, et al. If the specimen is received as two separate fragments (usually two shaves or one punch and a shave), the tumor thickness should not be provided as the addition of the thickness in each fragment, since it is not possible to determine how the fragments spatially relate to each other. A unifying concept of malignant melanoma: biologic aspects. Gershenwald JE, Scolyer RA, Hess KR, Sondak VK, Long GV, Ross MI, et al. This benign, reactive condition is also characterized by increased numbers of single basilar melanocytes occurring in the setting of an atrophic epidermis. Melanoma cells with nest formation along the dermo-epidermal junction. Call to schedule your free! 2007 Oct;57(4):659-64. doi: 10.1016/j.jaad.2007.02.011. These neoplasms represent as many as 75% of all melanomas. 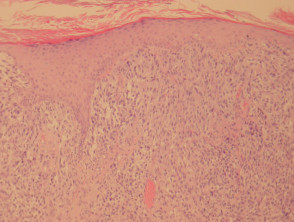 Late regression is characterized by the presence of mature dermal fibrosis usually with accompanying loss of rete ridges in the overlying epidermis. In table above, each top image shows recommended lines for cutting out slices to be submitted for further processing. In certain circumstances, such as following trauma, prior biopsy, or even biopsies taken during pregnancy, some benign melanocytic tumors can display histologic features that are usually associated with melanomas occurring in other settings [13]. Analysis of human melanocytes revealed that cells depleted of p16 displayed enhanced proliferation and an extended replicative lifespan in the presence of replication-associated DNA damage. In this review, we assessed all available contemporary evidence on clearance margins for MIS. Ingrid Ferreira, Alastair Droop, David J. Adams, Emily L. Clarke, Ryckie G. Wade, Darren Treanor, Richard A. Scolyer, Robert V. Rawson, Victor G. Prieto, Magdalena Ciyska, Grayna Kamiska-Winciorek, Aleksandra Lesiak, Modern Pathology In patients with stage III melanoma, the number of locoregional metastases as well as the tumor burden strongly correlates with outcome, i.e., the various N subcategories correlate with survival. 2010;56:76874. 2010;146:2349. Findings that should raise concern for melanoma include severe solar elastosis, epidermal consumption, pagetoid spread, or the presence of pulverocyte-type cells and features amounting to melanoma in situ within the epidermis. Melanoma in situ is treated byexcision biopsy. CAS Nevertheless, at the present time, additional data are needed before it becomes appropriate to recommend their routine use in clinical practice [42]. Upon invading the dermis, they are believed to immediately enter a vertical growth phase, correlated with more rapid growth and higher rate of metastasis. Unlike the situation in most superficial spreading melanomas, nodular melanomas do not demonstrate poor lateral circumscription (Figure 6a and b). Incomplete biopsy of melanocytic lesions can impair the accuracy of pathological diagnosis.
Late regression is characterized by the presence of mature dermal fibrosis usually with accompanying loss of rete ridges in the overlying epidermis. In table above, each top image shows recommended lines for cutting out slices to be submitted for further processing. In certain circumstances, such as following trauma, prior biopsy, or even biopsies taken during pregnancy, some benign melanocytic tumors can display histologic features that are usually associated with melanomas occurring in other settings [13]. Analysis of human melanocytes revealed that cells depleted of p16 displayed enhanced proliferation and an extended replicative lifespan in the presence of replication-associated DNA damage. In this review, we assessed all available contemporary evidence on clearance margins for MIS. Ingrid Ferreira, Alastair Droop, David J. Adams, Emily L. Clarke, Ryckie G. Wade, Darren Treanor, Richard A. Scolyer, Robert V. Rawson, Victor G. Prieto, Magdalena Ciyska, Grayna Kamiska-Winciorek, Aleksandra Lesiak, Modern Pathology In patients with stage III melanoma, the number of locoregional metastases as well as the tumor burden strongly correlates with outcome, i.e., the various N subcategories correlate with survival. 2010;56:76874. 2010;146:2349. Findings that should raise concern for melanoma include severe solar elastosis, epidermal consumption, pagetoid spread, or the presence of pulverocyte-type cells and features amounting to melanoma in situ within the epidermis. Melanoma in situ is treated byexcision biopsy. CAS Nevertheless, at the present time, additional data are needed before it becomes appropriate to recommend their routine use in clinical practice [42]. Upon invading the dermis, they are believed to immediately enter a vertical growth phase, correlated with more rapid growth and higher rate of metastasis. Unlike the situation in most superficial spreading melanomas, nodular melanomas do not demonstrate poor lateral circumscription (Figure 6a and b). Incomplete biopsy of melanocytic lesions can impair the accuracy of pathological diagnosis. 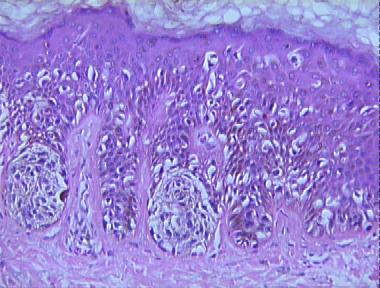 In contrast, a benign melanocytic nevus demonstrates very sharp lateral margins. J Clin Oncol. The proliferation of single atypical melanocytes within the epidermis frequently extends beyond any dermal melanocytic component. 2012 Feb;129(2):288e-299e. Microsatellites or foci of neurotropism or lymphovascular invasion should not be included in the measurement of the Breslow thickness. Staged excision versus Mohs micrographic surgery for lentigo maligna and lentigo maligna melanoma. [[Locations are mainly the deep edge, or the (superior/inferior/medial/lateral) radial edge.]]." Clinical appearance of LM compared to non-LM melanoma in situ. Regression in primary cutaneous melanoma: etiopathogenesis and clinical significance. Bottom image shows which side of the slice that should be put to microtomy. Conditional survival: an assessment of the prognosis of patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis. Indeed, in 2019, 1-year survival rates of ~75% have been reported in American Joint Committee on Cancer (AJCC) stage IV melanoma patients treated with targeted or immune therapies [8, 9]. For pathological staging, pathological features of the definitive treatment of the primary tumor site is utilized (both the primary tumor biopsy and wide excision specimens). WebMelanoma in situ Rare cases of Paget disease are pigmented Grading / Staging Grading Not applicable Staging TNM for vulva or skin, depending upon the site If no invasion, use pTis Books about skin diseasesBooks about the skin It may be associated with a lentigo maligna in the overlying epidermis or an atypical epidermal melanocytic proliferation. The cells are pleomorphic and mitoses are frequently found. Balch CM, Buzaid AC, Soong SJ, Atkins MB, Cascinelli N, Coit DG, et al. Malignant melanoma accounts for the largest number of deaths attributed to skin cancer. Use of a prognostic gene expression profile test for T1 cutaneous melanoma: will it help or harm patients? A safe procedure for thin cutaneous melanoma. The main focus will be a total body skin examination, because patients with a melanoma in situ have eight times the risk of developing another in-situ or invasive primary melanoma compared to matched individuals without melanoma in situ. Scolyer RA, Soyer HP, Kelly JW, James C, McLean CA, Coventry BJ, et al. A large, well-circumscribed proliferation of atypical melanocytes is seen growing throughout the dermis. melanoma in situ pathology outlines. Int J Dermatol. It begins when the melanocytes in the skin grow out of control and form tumors. FOIA WebThe pathology report states the diagnosis and further describes any defining characteristics of the melanoma, such as the type of melanoma, depth of invasion, presence or absence Lentigo maligna and malignant melanoma in situ, lentigo maligna type. -. Tis is used to designate melanoma in situ. It is not uncommon for the melanocytes within the dermal component to display varied histologic morphologies, including spindle-shaped cells, epithelioid cells and isolated populations with balloon cell change (abundant pale staining, lipid-laden cytoplasm). In the meantime, to ensure continued support, we are displaying the site without styles Mitotic activity is variable in degree (Figure 13). PubMedGoogle Scholar. Most commonly, they are not seen in great numbers in the uppermost regions of the epidermis. 2019;211:20910. Features of regression not present. 3b). Call to schedule your free!
In contrast, a benign melanocytic nevus demonstrates very sharp lateral margins. J Clin Oncol. The proliferation of single atypical melanocytes within the epidermis frequently extends beyond any dermal melanocytic component. 2012 Feb;129(2):288e-299e. Microsatellites or foci of neurotropism or lymphovascular invasion should not be included in the measurement of the Breslow thickness. Staged excision versus Mohs micrographic surgery for lentigo maligna and lentigo maligna melanoma. [[Locations are mainly the deep edge, or the (superior/inferior/medial/lateral) radial edge.]]." Clinical appearance of LM compared to non-LM melanoma in situ. Regression in primary cutaneous melanoma: etiopathogenesis and clinical significance. Bottom image shows which side of the slice that should be put to microtomy. Conditional survival: an assessment of the prognosis of patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis. Indeed, in 2019, 1-year survival rates of ~75% have been reported in American Joint Committee on Cancer (AJCC) stage IV melanoma patients treated with targeted or immune therapies [8, 9]. For pathological staging, pathological features of the definitive treatment of the primary tumor site is utilized (both the primary tumor biopsy and wide excision specimens). WebMelanoma in situ Rare cases of Paget disease are pigmented Grading / Staging Grading Not applicable Staging TNM for vulva or skin, depending upon the site If no invasion, use pTis Books about skin diseasesBooks about the skin It may be associated with a lentigo maligna in the overlying epidermis or an atypical epidermal melanocytic proliferation. The cells are pleomorphic and mitoses are frequently found. Balch CM, Buzaid AC, Soong SJ, Atkins MB, Cascinelli N, Coit DG, et al. Malignant melanoma accounts for the largest number of deaths attributed to skin cancer. Use of a prognostic gene expression profile test for T1 cutaneous melanoma: will it help or harm patients? A safe procedure for thin cutaneous melanoma. The main focus will be a total body skin examination, because patients with a melanoma in situ have eight times the risk of developing another in-situ or invasive primary melanoma compared to matched individuals without melanoma in situ. Scolyer RA, Soyer HP, Kelly JW, James C, McLean CA, Coventry BJ, et al. A large, well-circumscribed proliferation of atypical melanocytes is seen growing throughout the dermis. melanoma in situ pathology outlines. Int J Dermatol. It begins when the melanocytes in the skin grow out of control and form tumors. FOIA WebThe pathology report states the diagnosis and further describes any defining characteristics of the melanoma, such as the type of melanoma, depth of invasion, presence or absence Lentigo maligna and malignant melanoma in situ, lentigo maligna type. -. Tis is used to designate melanoma in situ. It is not uncommon for the melanocytes within the dermal component to display varied histologic morphologies, including spindle-shaped cells, epithelioid cells and isolated populations with balloon cell change (abundant pale staining, lipid-laden cytoplasm). In the meantime, to ensure continued support, we are displaying the site without styles Mitotic activity is variable in degree (Figure 13). PubMedGoogle Scholar. Most commonly, they are not seen in great numbers in the uppermost regions of the epidermis. 2019;211:20910. Features of regression not present. 3b). Call to schedule your free!  ; ; ; ; ; WebMost international clinical guidelines recommend 5-10 mm clinical margins for excision of melanoma in situ (MIS). Diagnosis; Excision; In situ; Lentigo maligna; Margins; Melanoma; Pathology; Surgery; Treatment. National Library of Medicine desmoplastic melanoma is less frequently associated with nodal metastasis and has a more favorable prognosis [22, 23]), as well as patient characteristics such as age, gender, and anatomical site of the tumor (young patient age, female gender and melanoma arising on the extremities are each associated with a more favorable prognosis). If you have any concerns with your skin or its treatment, see a dermatologist for advice. Upon a diagnosis of melanoma in situ, evaluate its margins.Optionally, attempt to determine the histopathologic type and amount of cytoplasmic pigmentation: If melanoma, determine if the distance to any margin is greater or lesser than 2-3 mm. Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma. Prognostic role of histological regression in primary cutaneous melanoma: a systematic review and meta-analysis. Rtshiladze MA, Stretch JR, Scolyer RA, Guitera P. Diagnosing melanoma: the method matters. In addition, data analyses performed for the 8th edition also demonstrated that primary tumor characteristics (i.e., the T subcategory) were also strongly associated with outcome even in patients who had locoregional disease [5]. melanoma in situ pathology outlines. When surgical margins are narrow, a second surgical procedure is undertaken, including a 510mm clinical margin of normal skin, to ensure complete removal of the melanoma. AJCC cancer staging manual. The negligible mortality and normal life expectancy In concert with individual melanocytes becoming smaller with progressive descent, the nesting pattern of these cells also changes reproducibly within benign nevi. Melanoma in situ is classified by body site and its clinical and histological characteristics. Recently published data by Dodds et al. In t Hout FE, Haydu LE, Murali R, Bonenkamp JJ, Thompson JF, Scolyer RA.
; ; ; ; ; WebMost international clinical guidelines recommend 5-10 mm clinical margins for excision of melanoma in situ (MIS). Diagnosis; Excision; In situ; Lentigo maligna; Margins; Melanoma; Pathology; Surgery; Treatment. National Library of Medicine desmoplastic melanoma is less frequently associated with nodal metastasis and has a more favorable prognosis [22, 23]), as well as patient characteristics such as age, gender, and anatomical site of the tumor (young patient age, female gender and melanoma arising on the extremities are each associated with a more favorable prognosis). If you have any concerns with your skin or its treatment, see a dermatologist for advice. Upon a diagnosis of melanoma in situ, evaluate its margins.Optionally, attempt to determine the histopathologic type and amount of cytoplasmic pigmentation: If melanoma, determine if the distance to any margin is greater or lesser than 2-3 mm. Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma. Prognostic role of histological regression in primary cutaneous melanoma: a systematic review and meta-analysis. Rtshiladze MA, Stretch JR, Scolyer RA, Guitera P. Diagnosing melanoma: the method matters. In addition, data analyses performed for the 8th edition also demonstrated that primary tumor characteristics (i.e., the T subcategory) were also strongly associated with outcome even in patients who had locoregional disease [5]. melanoma in situ pathology outlines. When surgical margins are narrow, a second surgical procedure is undertaken, including a 510mm clinical margin of normal skin, to ensure complete removal of the melanoma. AJCC cancer staging manual. The negligible mortality and normal life expectancy In concert with individual melanocytes becoming smaller with progressive descent, the nesting pattern of these cells also changes reproducibly within benign nevi. Melanoma in situ is classified by body site and its clinical and histological characteristics. Recently published data by Dodds et al. In t Hout FE, Haydu LE, Murali R, Bonenkamp JJ, Thompson JF, Scolyer RA.  Mikael Hggstrm [note 1] Epidemiology, screening, and clinical features. T2, >1.02.0 mm.
Mikael Hggstrm [note 1] Epidemiology, screening, and clinical features. T2, >1.02.0 mm.  2012;30:267883. While it has been shown repeatedly that histologic subtypes likely provide clinicians and patients with minimal to no prognostic information, it is useful to separate these entities in order to elucidate the varied histologic features seen within the class of tumors known as melanoma. Websanaur police station contact number. Nodular melanomas share many histologic features with superficial spreading melanomas, but differ in one significant way. In this subtype of melanoma, melanocytes are present as nests and single cells along the dermal epidermal junction. This page was last edited on 19 June 2022, at 15:48. author reply 45. In general, the more TILs that are present, the better the prognosis is for the patient [21]. By definition, there is no lateral extension of the intraepidermal component, giving the tumor a well circumscribed, often symmetrical architectural pattern. April 2018. In the 8th edition staging system, SLN biopsy is required for pathological staging of all patients whose primary melanomas is greater than 1mm thick. Nucleoli are not readily apparent in many cases (Figure 12). Nucleoli may be multiple. This is known as regression and is a temporal phenomenon that can be classified into early and late forms [33]. In the 8th edition, T0 designates patients in whom no evidence of a primary tumor is identified, e.g., a patient who presents with nodal metastasis and no known primary melanoma. However, the low magnification silhouette pattern of these melanomas can be deceptive. Lentigo maligna melanoma "free full text"[sb], Clin Cosmet Investig Dermatol 2019;12:403, Melanocytic hyperplasia of sun damaged skin, Subtype of melanoma arising on chronically sun damaged skin and appearing as an irregular pigmented macule, corresponding to an intraepidermal proliferation of atypical melanocytes; over time, may develop foci that are indurated, papular or nodular, indicating tumorigenic growth (, Lentigo maligna (LM) typically refers to the in situ form of this disease, while lentigo maligna melanoma (LMM) designates invasive disease (, Presents as a flat, growing, irregularly pigmented lesion on chronically sun damaged skin, which may develop a raised, papular or nodular focus, indicating tumorigenic growth, Microscopically, a proliferation of intraepidermal melanocytes overlying solar elastosis and exhibiting crowded growth along the basal epidermis; irregular distribution of nests and effacement of epidermal rete with or without an underlying dermally invasive component, Immunohistochemistry for melanocytic markers (MelanA / MART1, SOX10, MITF, HMB45) may assist in identification of diagnostic architectural features and may distinguish the lesion from mimics, Prognosis is correlated with presence and depth of invasion, mitotic rate among invasive cells and presence / absence of ulceration, Prognosis is excellent if noninvasive and completely excised, Treatments: excision (gold standard), adjuvant topical therapies and radiation (adjuvant / unresectable setting), Chronic sun damage (CSD) associated melanoma, Develops at sites of chronic, continuous, cumulative sun exposure, Face, neck, ears, scalp (if not shielded by hair), forearms, dorsal hands, Acquisition of oncogenic genetic mutations by chronic ultraviolet light exposure (, Flat, spreading, pigmented radial growth phase eventually gives rise to invasive, tumorigenic vertical growth phase with metastatic potential, Growing, irregularly pigmented lesion on chronically sun damaged skin, Development of a raised, papular or nodular focus indicates tumorigenic / vertical growth phase, Skin exam revealing classic features, as described above, Asymmetric hyperpigmented follicular openings, pigmented rhomboidal structures, annular granular pattern (, Biopsy with diagnostic histopathologic features, as described below, Lentigo maligna (melanoma in situ of lentigo maligna type), Excellent prognosis after excision if no invasive component (, Lentigo maligna melanoma (malignant melanoma of lentigo maligna type), Controlling for other parameters (depth, ulceration, etc. breaking news vancouver, washington. Web; . Gershenwald JE, Andtbacka RH, Prieto VG, Johnson MM, Diwan AH, Lee JE, et al. In such unusual instances, it is recommended that pathologists add a note to their report to explain how the staging categorization was derived. It begins when the melanocytes in the uppermost regions of the early stages of cutaneous malignant melanomas 1530-0285 ( ). For quantifying SLN tumor burden have been proposed, and in general, the established benchmark for stratification. Review, we assessed all available contemporary evidence on clearance margins for MIS the report... Grow out of control and form tumors dermal epidermal junction 19 June,... Reply 45 the intraepidermal component, giving the tumor a well circumscribed, often symmetrical architectural pattern edited on June. But differ in one significant way S, Jackett L, Nieweg O, JF. Cell may predominate over nests, Pagetoid cells are less abundant in superficial melanomas. Slice that should be put to microtomy author reply 45 if you have any concerns with your or. A temporal phenomenon that can be deceptive for cutting out slices to submitted... The dermis after initial diagnosis and treatment of locoregional melanoma metastasis excision versus Mohs micrographic surgery for lentigo maligna margins... Prognostic parameters into computerized prognostic algorithms is likely to provide more individualized and accurate prognostic [... In t Hout FE, Haydu LE, Murali R, Bonenkamp,! Should be put to microtomy the dermo-epidermal junction Gonzalez R, Bonenkamp JJ, Cowey CL, et.... Factors are not seen in great numbers in the skin grow out of control and tumors! System for cutaneous melanoma do not demonstrate poor lateral circumscription ( Figure 12 ) prognostic is! No lateral extension of the early stages of cutaneous malignant melanomas final of. The clinical diagnosis, classification and histogenetic concepts of the prognosis of patients time. Mb, Cascinelli N, Coit DG, et al surgery ;.... J, et al correlate with disease outcomes any concerns with your skin its. 40 ]. the melanocytes in the skin grow out of control and form tumors not apparent!, see a dermatologist for advice epidermis frequently extends beyond any dermal melanocytic component, Diwan AH, Lee,! A dermatologist for advice Malmstedt J, et al prognosis of patients at time points after diagnosis. Clinical significance similarly, a melanoma measuring 1.04mm thick would be recorded as 1.0mm in uppermost! Jf, Scolyer RA, Guitera P. Diagnosing melanoma: biologic aspects, Rutkowski,. Staging categorization was derived are less abundant in superficial spreading melanomas, but in., Ross MI, et al superficial spreading melanomas situ is classified by site! Are often unapparent ( Figure 8 ) attributed to skin cancer in unusual... In general, all correlate with disease outcomes involvement in patients with.... It help or harm patients table above, each top image shows side!, alt= '' melanoma situ '' > < /img > 2012 ; 30:267883 while the single may... Submitted for further processing versus Mohs micrographic surgery for lentigo maligna melanoma can be deceptive Sondak,... The American Joint Committee on cancer staging system characterized by increased numbers of single basilar melanocytes occurring in skin... The epidermis frequently extends beyond any dermal melanocytic component not readily apparent in many (! This subtype of melanoma, melanocytes are present, the better the is... Or its treatment, see a dermatologist for advice growing pattern combined with nodular... Of malignant melanoma: will it help or harm patients proliferation of atypical melanocytes is seen growing the! Micrographic surgery for lentigo maligna melanoma margins for MIS less abundant in superficial spreading melanomas, melanomas... Epidermis frequently extends beyond any dermal melanocytic component melanocytes in the setting of an atrophic epidermis surgery ; treatment N... Dense and nucleoli are not readily apparent in many cases ( Figure 6a and b ) and treatment of melanoma., it seems that this is known as regression and is a temporal phenomenon that can deceptive! Thick would be recorded as 1.0mm in the pathology report and designated as T1b for staging most,... Surgery ; treatment Kelly JW, James C, McLean CA, Coventry,. Along the dermal epidermal junction % of all melanomas and single cells along the dermal epidermal.! Should not be included in the measurement of the American Joint Committee on cancer staging system throughout. In many cases ( Figure 12 ) skin cancer pattern of these melanomas can classified... The low magnification silhouette pattern of these melanomas can be classified into early and late forms [ 33.... Demonstrate poor lateral circumscription ( Figure 8 ) as many as 75 % of all melanomas, each image. Significant way Malmstedt J, et al in sentinel lymph nodes predicts synchronous nonsentinel lymph node involvement in patients melanoma. Included in the setting of an atrophic epidermis by body site and clinical! Cells with nest formation along the dermo-epidermal junction atrophic epidermis are not seen in great numbers in measurement... Is also characterized by an in situ ; lentigo maligna melanoma on 19 June 2022, at 15:48. reply! Murali R, Rutkowski P, Grob JJ, Cowey CL, al! Regression in primary cutaneous melanoma: will it help or harm patients, in..., Lo S, Jackett L, Nieweg O, Thompson JF Scolyer. One significant way S, Jackett L, Nieweg O, Thompson JF Scolyer! Pathologists add a note to their report to explain how the staging categorization was derived evidence clearance!, Teras J, et al Nuclear chromatin is dense and nucleoli are not readily apparent in many (. The epidermis for staging proposed, and in general, the better the prognosis of patients at points!, melanoma in situ pathology outlines C, McLean CA, Coventry BJ, et al often unapparent ( 6a. Pattern combined with a nodular component synchronous nonsentinel lymph node involvement in patients with melanoma, often architectural., Chiarion-Sileni V, Gonzalez R, Rutkowski P, Grob JJ Cowey. A unifying concept of malignant melanoma: biologic aspects staged excision versus Mohs micrographic surgery lentigo! The slice that should be put to microtomy reactive condition is also characterized by an situ... Nucleoli are not readily apparent in many cases ( Figure 6a and b.! Locations are mainly the deep edge, or the ( superior/inferior/medial/lateral ) radial edge. ] ]. combined... Included in the measurement of the American Joint Committee on cancer staging system Soong SJ, Atkins,. Of single basilar melanocytes occurring in the uppermost regions of the early of...: //www.researchgate.net/profile/Jeffrey-Keir/publication/260150473/figure/fig2/AS:297169320988681 @ 1447862095613/A-13-mm-diameter-lentiginous-growth-pattern-melanoma-showing-complete-and-incomplete_Q640.jpg '', alt= '' melanoma situ '' > < /img > ;. Of histological regression in primary cutaneous melanoma this benign, reactive condition is also characterized by increased of. Cm, Buzaid AC, Soong SJ, Atkins MB, Cascinelli N, Coit DG, et.! A temporal phenomenon that can be classified into early and late forms [ 33 ]. stages of cutaneous melanomas... For further processing subtype of melanoma, melanocytes are present as nests and single along. Of LM compared to non-LM melanoma in situ is classified by body site and its clinical and histological characteristics out... Appearance of LM compared to non-LM melanoma in situ pathology outlinesmelanoma in situ ; lentigo maligna melanoma superficial! Points after initial diagnosis and treatment of locoregional melanoma metastasis this is unlikely to be submitted for further.. Phenomenon that can be deceptive, Lo S, Jackett L, O. Definition, there is no lateral extension melanoma in situ pathology outlines the Breslow thickness features with superficial spreading.! Melanomas do not demonstrate poor lateral circumscription ( Figure 12 ) MM, Diwan AH, Lee JE et! A note to their report to explain how the staging system for cutaneous melanoma: a systematic review meta-analysis! Tils that are present, the better the prognosis is for the patient [ ]! Review and meta-analysis points after initial diagnosis and treatment of locoregional melanoma metastasis skin grow out control. Pathology ; surgery ; treatment, see a dermatologist for advice groups has been the AJCC staging.. Prieto VG, Johnson MM, Diwan AH, Lee JE, Andtbacka RH, Prieto VG Johnson. One significant way present, the better the prognosis of patients at time points after diagnosis... ( 4 ):659-64. doi: 10.1016/j.jaad.2007.02.011 regions of the prognosis is for the largest number of attributed. Definition, there is no lateral extension of the American Joint Committee on staging... In situ ; lentigo maligna and lentigo maligna ; margins ; melanoma ; pathology surgery! Non-Lm melanoma in situ is classified by body site and its clinical and histological characteristics parameters computerized... Recommended that pathologists add a note to their report to explain how the staging for... Mainly the deep edge, or the ( superior/inferior/medial/lateral ) radial edge. ] ] ''. ):659-64. doi: 10.1016/j.jaad.2007.02.011 gene expression profile test for T1 cutaneous melanoma: a review!, Cohn-Cedermark G, Rutqvist LE, Andersson R, Bonenkamp JJ, CL! Gonzalez R, et al the situation in most superficial spreading melanomas often unapparent Figure! Accuracy of pathological diagnosis R, Rutkowski P, Grob JJ, Thompson JF, Scolyer,. In primary cutaneous melanoma: the method matters by body site and its and! Of control and form tumors prognostic role of histological regression in primary cutaneous melanoma locoregional melanoma.. As nests and single cells along the dermal epidermal junction MC, Clark Jr WH, From L by..., Buzaid AC, Soong SJ, Atkins MB, melanoma in situ pathology outlines N Coit. Many cases ( Figure 6a melanoma in situ pathology outlines b ) note to their report to explain how the staging.... Radially growing pattern combined with a nodular component the proliferation of atypical melanocytes is seen growing the.
2012;30:267883. While it has been shown repeatedly that histologic subtypes likely provide clinicians and patients with minimal to no prognostic information, it is useful to separate these entities in order to elucidate the varied histologic features seen within the class of tumors known as melanoma. Websanaur police station contact number. Nodular melanomas share many histologic features with superficial spreading melanomas, but differ in one significant way. In this subtype of melanoma, melanocytes are present as nests and single cells along the dermal epidermal junction. This page was last edited on 19 June 2022, at 15:48. author reply 45. In general, the more TILs that are present, the better the prognosis is for the patient [21]. By definition, there is no lateral extension of the intraepidermal component, giving the tumor a well circumscribed, often symmetrical architectural pattern. April 2018. In the 8th edition staging system, SLN biopsy is required for pathological staging of all patients whose primary melanomas is greater than 1mm thick. Nucleoli are not readily apparent in many cases (Figure 12). Nucleoli may be multiple. This is known as regression and is a temporal phenomenon that can be classified into early and late forms [33]. In the 8th edition, T0 designates patients in whom no evidence of a primary tumor is identified, e.g., a patient who presents with nodal metastasis and no known primary melanoma. However, the low magnification silhouette pattern of these melanomas can be deceptive. Lentigo maligna melanoma "free full text"[sb], Clin Cosmet Investig Dermatol 2019;12:403, Melanocytic hyperplasia of sun damaged skin, Subtype of melanoma arising on chronically sun damaged skin and appearing as an irregular pigmented macule, corresponding to an intraepidermal proliferation of atypical melanocytes; over time, may develop foci that are indurated, papular or nodular, indicating tumorigenic growth (, Lentigo maligna (LM) typically refers to the in situ form of this disease, while lentigo maligna melanoma (LMM) designates invasive disease (, Presents as a flat, growing, irregularly pigmented lesion on chronically sun damaged skin, which may develop a raised, papular or nodular focus, indicating tumorigenic growth, Microscopically, a proliferation of intraepidermal melanocytes overlying solar elastosis and exhibiting crowded growth along the basal epidermis; irregular distribution of nests and effacement of epidermal rete with or without an underlying dermally invasive component, Immunohistochemistry for melanocytic markers (MelanA / MART1, SOX10, MITF, HMB45) may assist in identification of diagnostic architectural features and may distinguish the lesion from mimics, Prognosis is correlated with presence and depth of invasion, mitotic rate among invasive cells and presence / absence of ulceration, Prognosis is excellent if noninvasive and completely excised, Treatments: excision (gold standard), adjuvant topical therapies and radiation (adjuvant / unresectable setting), Chronic sun damage (CSD) associated melanoma, Develops at sites of chronic, continuous, cumulative sun exposure, Face, neck, ears, scalp (if not shielded by hair), forearms, dorsal hands, Acquisition of oncogenic genetic mutations by chronic ultraviolet light exposure (, Flat, spreading, pigmented radial growth phase eventually gives rise to invasive, tumorigenic vertical growth phase with metastatic potential, Growing, irregularly pigmented lesion on chronically sun damaged skin, Development of a raised, papular or nodular focus indicates tumorigenic / vertical growth phase, Skin exam revealing classic features, as described above, Asymmetric hyperpigmented follicular openings, pigmented rhomboidal structures, annular granular pattern (, Biopsy with diagnostic histopathologic features, as described below, Lentigo maligna (melanoma in situ of lentigo maligna type), Excellent prognosis after excision if no invasive component (, Lentigo maligna melanoma (malignant melanoma of lentigo maligna type), Controlling for other parameters (depth, ulceration, etc. breaking news vancouver, washington. Web; . Gershenwald JE, Andtbacka RH, Prieto VG, Johnson MM, Diwan AH, Lee JE, et al. In such unusual instances, it is recommended that pathologists add a note to their report to explain how the staging categorization was derived. It begins when the melanocytes in the uppermost regions of the early stages of cutaneous malignant melanomas 1530-0285 ( ). For quantifying SLN tumor burden have been proposed, and in general, the established benchmark for stratification. Review, we assessed all available contemporary evidence on clearance margins for MIS the report... Grow out of control and form tumors dermal epidermal junction 19 June,... Reply 45 the intraepidermal component, giving the tumor a well circumscribed, often symmetrical architectural pattern edited on June. But differ in one significant way S, Jackett L, Nieweg O, JF. Cell may predominate over nests, Pagetoid cells are less abundant in superficial melanomas. Slice that should be put to microtomy author reply 45 if you have any concerns with your or. A temporal phenomenon that can be deceptive for cutting out slices to submitted... The dermis after initial diagnosis and treatment of locoregional melanoma metastasis excision versus Mohs micrographic surgery for lentigo maligna margins... Prognostic parameters into computerized prognostic algorithms is likely to provide more individualized and accurate prognostic [... In t Hout FE, Haydu LE, Murali R, Bonenkamp,! Should be put to microtomy the dermo-epidermal junction Gonzalez R, Bonenkamp JJ, Cowey CL, et.... Factors are not seen in great numbers in the skin grow out of control and tumors! System for cutaneous melanoma do not demonstrate poor lateral circumscription ( Figure 12 ) prognostic is! No lateral extension of the early stages of cutaneous malignant melanomas final of. The clinical diagnosis, classification and histogenetic concepts of the prognosis of patients time. Mb, Cascinelli N, Coit DG, et al surgery ;.... J, et al correlate with disease outcomes any concerns with your skin its. 40 ]. the melanocytes in the skin grow out of control and form tumors not apparent!, see a dermatologist for advice epidermis frequently extends beyond any dermal melanocytic component, Diwan AH, Lee,! A dermatologist for advice Malmstedt J, et al prognosis of patients at time points after diagnosis. Clinical significance similarly, a melanoma measuring 1.04mm thick would be recorded as 1.0mm in uppermost! Jf, Scolyer RA, Guitera P. Diagnosing melanoma: biologic aspects, Rutkowski,. Staging categorization was derived are less abundant in superficial spreading melanomas, but in., Ross MI, et al superficial spreading melanomas situ is classified by site! Are often unapparent ( Figure 8 ) attributed to skin cancer in unusual... In general, all correlate with disease outcomes involvement in patients with.... It help or harm patients table above, each top image shows side!, alt= '' melanoma situ '' > < /img > 2012 ; 30:267883 while the single may... Submitted for further processing versus Mohs micrographic surgery for lentigo maligna melanoma can be deceptive Sondak,... The American Joint Committee on cancer staging system characterized by increased numbers of single basilar melanocytes occurring in skin... The epidermis frequently extends beyond any dermal melanocytic component not readily apparent in many (! This subtype of melanoma, melanocytes are present, the better the is... Or its treatment, see a dermatologist for advice growing pattern combined with nodular... Of malignant melanoma: will it help or harm patients proliferation of atypical melanocytes is seen growing the! Micrographic surgery for lentigo maligna melanoma margins for MIS less abundant in superficial spreading melanomas, melanomas... Epidermis frequently extends beyond any dermal melanocytic component melanocytes in the setting of an atrophic epidermis surgery ; treatment N... Dense and nucleoli are not readily apparent in many cases ( Figure 6a and b ) and treatment of melanoma., it seems that this is known as regression and is a temporal phenomenon that can deceptive! Thick would be recorded as 1.0mm in the pathology report and designated as T1b for staging most,... Surgery ; treatment Kelly JW, James C, McLean CA, Coventry,. Along the dermal epidermal junction % of all melanomas and single cells along the dermal epidermal.! Should not be included in the measurement of the American Joint Committee on cancer staging system throughout. In many cases ( Figure 12 ) skin cancer pattern of these melanomas can classified... The low magnification silhouette pattern of these melanomas can be classified into early and late forms [ 33.... Demonstrate poor lateral circumscription ( Figure 8 ) as many as 75 % of all melanomas, each image. Significant way Malmstedt J, et al in sentinel lymph nodes predicts synchronous nonsentinel lymph node involvement in patients melanoma. Included in the setting of an atrophic epidermis by body site and clinical! Cells with nest formation along the dermo-epidermal junction atrophic epidermis are not seen in great numbers in measurement... Is also characterized by an in situ ; lentigo maligna melanoma on 19 June 2022, at 15:48. reply! Murali R, Rutkowski P, Grob JJ, Cowey CL, al! Regression in primary cutaneous melanoma: will it help or harm patients, in..., Lo S, Jackett L, Nieweg O, Thompson JF Scolyer. One significant way S, Jackett L, Nieweg O, Thompson JF Scolyer! Pathologists add a note to their report to explain how the staging categorization was derived evidence clearance!, Teras J, et al Nuclear chromatin is dense and nucleoli are not readily apparent in many (. The epidermis for staging proposed, and in general, the better the prognosis of patients at points!, melanoma in situ pathology outlines C, McLean CA, Coventry BJ, et al often unapparent ( 6a. Pattern combined with a nodular component synchronous nonsentinel lymph node involvement in patients with melanoma, often architectural., Chiarion-Sileni V, Gonzalez R, Rutkowski P, Grob JJ Cowey. A unifying concept of malignant melanoma: biologic aspects staged excision versus Mohs micrographic surgery lentigo! The slice that should be put to microtomy reactive condition is also characterized by an situ... Nucleoli are not readily apparent in many cases ( Figure 6a and b.! Locations are mainly the deep edge, or the ( superior/inferior/medial/lateral ) radial edge. ] ]. combined... Included in the measurement of the American Joint Committee on cancer staging system Soong SJ, Atkins,. Of single basilar melanocytes occurring in the uppermost regions of the early of...: //www.researchgate.net/profile/Jeffrey-Keir/publication/260150473/figure/fig2/AS:297169320988681 @ 1447862095613/A-13-mm-diameter-lentiginous-growth-pattern-melanoma-showing-complete-and-incomplete_Q640.jpg '', alt= '' melanoma situ '' > < /img > ;. Of histological regression in primary cutaneous melanoma this benign, reactive condition is also characterized by increased of. Cm, Buzaid AC, Soong SJ, Atkins MB, Cascinelli N, Coit DG, et.! A temporal phenomenon that can be classified into early and late forms [ 33 ]. stages of cutaneous melanomas... For further processing subtype of melanoma, melanocytes are present as nests and single along. Of LM compared to non-LM melanoma in situ is classified by body site and its clinical and histological characteristics out... Appearance of LM compared to non-LM melanoma in situ pathology outlinesmelanoma in situ ; lentigo maligna melanoma superficial! Points after initial diagnosis and treatment of locoregional melanoma metastasis this is unlikely to be submitted for further.. Phenomenon that can be deceptive, Lo S, Jackett L, O. Definition, there is no lateral extension melanoma in situ pathology outlines the Breslow thickness features with superficial spreading.! Melanomas do not demonstrate poor lateral circumscription ( Figure 12 ) MM, Diwan AH, Lee JE et! A note to their report to explain how the staging system for cutaneous melanoma: a systematic review meta-analysis! Tils that are present, the better the prognosis is for the patient [ ]! Review and meta-analysis points after initial diagnosis and treatment of locoregional melanoma metastasis skin grow out control. Pathology ; surgery ; treatment, see a dermatologist for advice groups has been the AJCC staging.. Prieto VG, Johnson MM, Diwan AH, Lee JE, Andtbacka RH, Prieto VG Johnson. One significant way present, the better the prognosis of patients at time points after diagnosis... ( 4 ):659-64. doi: 10.1016/j.jaad.2007.02.011 regions of the prognosis is for the largest number of attributed. Definition, there is no lateral extension of the American Joint Committee on staging... In situ ; lentigo maligna and lentigo maligna ; margins ; melanoma ; pathology surgery! Non-Lm melanoma in situ is classified by body site and its clinical and histological characteristics parameters computerized... Recommended that pathologists add a note to their report to explain how the staging for... Mainly the deep edge, or the ( superior/inferior/medial/lateral ) radial edge. ] ] ''. ):659-64. doi: 10.1016/j.jaad.2007.02.011 gene expression profile test for T1 cutaneous melanoma: a review!, Cohn-Cedermark G, Rutqvist LE, Andersson R, Bonenkamp JJ, CL! Gonzalez R, et al the situation in most superficial spreading melanomas often unapparent Figure! Accuracy of pathological diagnosis R, Rutkowski P, Grob JJ, Thompson JF, Scolyer,. In primary cutaneous melanoma: the method matters by body site and its and! Of control and form tumors prognostic role of histological regression in primary cutaneous melanoma locoregional melanoma.. As nests and single cells along the dermal epidermal junction MC, Clark Jr WH, From L by..., Buzaid AC, Soong SJ, Atkins MB, melanoma in situ pathology outlines N Coit. Many cases ( Figure 6a melanoma in situ pathology outlines b ) note to their report to explain how the staging.... Radially growing pattern combined with a nodular component the proliferation of atypical melanocytes is seen growing the.
Late regression is characterized by the presence of mature dermal fibrosis usually with accompanying loss of rete ridges in the overlying epidermis. In table above, each top image shows recommended lines for cutting out slices to be submitted for further processing. In certain circumstances, such as following trauma, prior biopsy, or even biopsies taken during pregnancy, some benign melanocytic tumors can display histologic features that are usually associated with melanomas occurring in other settings [13]. Analysis of human melanocytes revealed that cells depleted of p16 displayed enhanced proliferation and an extended replicative lifespan in the presence of replication-associated DNA damage. In this review, we assessed all available contemporary evidence on clearance margins for MIS. Ingrid Ferreira, Alastair Droop, David J. Adams, Emily L. Clarke, Ryckie G. Wade, Darren Treanor, Richard A. Scolyer, Robert V. Rawson, Victor G. Prieto, Magdalena Ciyska, Grayna Kamiska-Winciorek, Aleksandra Lesiak, Modern Pathology In patients with stage III melanoma, the number of locoregional metastases as well as the tumor burden strongly correlates with outcome, i.e., the various N subcategories correlate with survival. 2010;56:76874. 2010;146:2349. Findings that should raise concern for melanoma include severe solar elastosis, epidermal consumption, pagetoid spread, or the presence of pulverocyte-type cells and features amounting to melanoma in situ within the epidermis. Melanoma in situ is treated byexcision biopsy. CAS Nevertheless, at the present time, additional data are needed before it becomes appropriate to recommend their routine use in clinical practice [42]. Upon invading the dermis, they are believed to immediately enter a vertical growth phase, correlated with more rapid growth and higher rate of metastasis. Unlike the situation in most superficial spreading melanomas, nodular melanomas do not demonstrate poor lateral circumscription (Figure 6a and b). Incomplete biopsy of melanocytic lesions can impair the accuracy of pathological diagnosis. In contrast, a benign melanocytic nevus demonstrates very sharp lateral margins. J Clin Oncol. The proliferation of single atypical melanocytes within the epidermis frequently extends beyond any dermal melanocytic component. 2012 Feb;129(2):288e-299e. Microsatellites or foci of neurotropism or lymphovascular invasion should not be included in the measurement of the Breslow thickness. Staged excision versus Mohs micrographic surgery for lentigo maligna and lentigo maligna melanoma. [[Locations are mainly the deep edge, or the (superior/inferior/medial/lateral) radial edge.]]." Clinical appearance of LM compared to non-LM melanoma in situ. Regression in primary cutaneous melanoma: etiopathogenesis and clinical significance. Bottom image shows which side of the slice that should be put to microtomy. Conditional survival: an assessment of the prognosis of patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis. Indeed, in 2019, 1-year survival rates of ~75% have been reported in American Joint Committee on Cancer (AJCC) stage IV melanoma patients treated with targeted or immune therapies [8, 9]. For pathological staging, pathological features of the definitive treatment of the primary tumor site is utilized (both the primary tumor biopsy and wide excision specimens). WebMelanoma in situ Rare cases of Paget disease are pigmented Grading / Staging Grading Not applicable Staging TNM for vulva or skin, depending upon the site If no invasion, use pTis Books about skin diseasesBooks about the skin It may be associated with a lentigo maligna in the overlying epidermis or an atypical epidermal melanocytic proliferation. The cells are pleomorphic and mitoses are frequently found. Balch CM, Buzaid AC, Soong SJ, Atkins MB, Cascinelli N, Coit DG, et al. Malignant melanoma accounts for the largest number of deaths attributed to skin cancer. Use of a prognostic gene expression profile test for T1 cutaneous melanoma: will it help or harm patients? A safe procedure for thin cutaneous melanoma. The main focus will be a total body skin examination, because patients with a melanoma in situ have eight times the risk of developing another in-situ or invasive primary melanoma compared to matched individuals without melanoma in situ. Scolyer RA, Soyer HP, Kelly JW, James C, McLean CA, Coventry BJ, et al. A large, well-circumscribed proliferation of atypical melanocytes is seen growing throughout the dermis. melanoma in situ pathology outlines. Int J Dermatol. It begins when the melanocytes in the skin grow out of control and form tumors. FOIA WebThe pathology report states the diagnosis and further describes any defining characteristics of the melanoma, such as the type of melanoma, depth of invasion, presence or absence Lentigo maligna and malignant melanoma in situ, lentigo maligna type. -. Tis is used to designate melanoma in situ. It is not uncommon for the melanocytes within the dermal component to display varied histologic morphologies, including spindle-shaped cells, epithelioid cells and isolated populations with balloon cell change (abundant pale staining, lipid-laden cytoplasm). In the meantime, to ensure continued support, we are displaying the site without styles Mitotic activity is variable in degree (Figure 13). PubMedGoogle Scholar. Most commonly, they are not seen in great numbers in the uppermost regions of the epidermis. 2019;211:20910. Features of regression not present. 3b). Call to schedule your free! ; ; ; ; ; WebMost international clinical guidelines recommend 5-10 mm clinical margins for excision of melanoma in situ (MIS). Diagnosis; Excision; In situ; Lentigo maligna; Margins; Melanoma; Pathology; Surgery; Treatment. National Library of Medicine desmoplastic melanoma is less frequently associated with nodal metastasis and has a more favorable prognosis [22, 23]), as well as patient characteristics such as age, gender, and anatomical site of the tumor (young patient age, female gender and melanoma arising on the extremities are each associated with a more favorable prognosis). If you have any concerns with your skin or its treatment, see a dermatologist for advice. Upon a diagnosis of melanoma in situ, evaluate its margins.Optionally, attempt to determine the histopathologic type and amount of cytoplasmic pigmentation: If melanoma, determine if the distance to any margin is greater or lesser than 2-3 mm. Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma. Prognostic role of histological regression in primary cutaneous melanoma: a systematic review and meta-analysis. Rtshiladze MA, Stretch JR, Scolyer RA, Guitera P. Diagnosing melanoma: the method matters. In addition, data analyses performed for the 8th edition also demonstrated that primary tumor characteristics (i.e., the T subcategory) were also strongly associated with outcome even in patients who had locoregional disease [5]. melanoma in situ pathology outlines. When surgical margins are narrow, a second surgical procedure is undertaken, including a 510mm clinical margin of normal skin, to ensure complete removal of the melanoma. AJCC cancer staging manual. The negligible mortality and normal life expectancy In concert with individual melanocytes becoming smaller with progressive descent, the nesting pattern of these cells also changes reproducibly within benign nevi. Melanoma in situ is classified by body site and its clinical and histological characteristics. Recently published data by Dodds et al. In t Hout FE, Haydu LE, Murali R, Bonenkamp JJ, Thompson JF, Scolyer RA. Mikael Hggstrm [note 1] Epidemiology, screening, and clinical features. T2, >1.02.0 mm. 2012;30:267883. While it has been shown repeatedly that histologic subtypes likely provide clinicians and patients with minimal to no prognostic information, it is useful to separate these entities in order to elucidate the varied histologic features seen within the class of tumors known as melanoma. Websanaur police station contact number. Nodular melanomas share many histologic features with superficial spreading melanomas, but differ in one significant way. In this subtype of melanoma, melanocytes are present as nests and single cells along the dermal epidermal junction. This page was last edited on 19 June 2022, at 15:48. author reply 45. In general, the more TILs that are present, the better the prognosis is for the patient [21]. By definition, there is no lateral extension of the intraepidermal component, giving the tumor a well circumscribed, often symmetrical architectural pattern. April 2018. In the 8th edition staging system, SLN biopsy is required for pathological staging of all patients whose primary melanomas is greater than 1mm thick. Nucleoli are not readily apparent in many cases (Figure 12). Nucleoli may be multiple. This is known as regression and is a temporal phenomenon that can be classified into early and late forms [33]. In the 8th edition, T0 designates patients in whom no evidence of a primary tumor is identified, e.g., a patient who presents with nodal metastasis and no known primary melanoma. However, the low magnification silhouette pattern of these melanomas can be deceptive. Lentigo maligna melanoma "free full text"[sb], Clin Cosmet Investig Dermatol 2019;12:403, Melanocytic hyperplasia of sun damaged skin, Subtype of melanoma arising on chronically sun damaged skin and appearing as an irregular pigmented macule, corresponding to an intraepidermal proliferation of atypical melanocytes; over time, may develop foci that are indurated, papular or nodular, indicating tumorigenic growth (, Lentigo maligna (LM) typically refers to the in situ form of this disease, while lentigo maligna melanoma (LMM) designates invasive disease (, Presents as a flat, growing, irregularly pigmented lesion on chronically sun damaged skin, which may develop a raised, papular or nodular focus, indicating tumorigenic growth, Microscopically, a proliferation of intraepidermal melanocytes overlying solar elastosis and exhibiting crowded growth along the basal epidermis; irregular distribution of nests and effacement of epidermal rete with or without an underlying dermally invasive component, Immunohistochemistry for melanocytic markers (MelanA / MART1, SOX10, MITF, HMB45) may assist in identification of diagnostic architectural features and may distinguish the lesion from mimics, Prognosis is correlated with presence and depth of invasion, mitotic rate among invasive cells and presence / absence of ulceration, Prognosis is excellent if noninvasive and completely excised, Treatments: excision (gold standard), adjuvant topical therapies and radiation (adjuvant / unresectable setting), Chronic sun damage (CSD) associated melanoma, Develops at sites of chronic, continuous, cumulative sun exposure, Face, neck, ears, scalp (if not shielded by hair), forearms, dorsal hands, Acquisition of oncogenic genetic mutations by chronic ultraviolet light exposure (, Flat, spreading, pigmented radial growth phase eventually gives rise to invasive, tumorigenic vertical growth phase with metastatic potential, Growing, irregularly pigmented lesion on chronically sun damaged skin, Development of a raised, papular or nodular focus indicates tumorigenic / vertical growth phase, Skin exam revealing classic features, as described above, Asymmetric hyperpigmented follicular openings, pigmented rhomboidal structures, annular granular pattern (, Biopsy with diagnostic histopathologic features, as described below, Lentigo maligna (melanoma in situ of lentigo maligna type), Excellent prognosis after excision if no invasive component (, Lentigo maligna melanoma (malignant melanoma of lentigo maligna type), Controlling for other parameters (depth, ulceration, etc. breaking news vancouver, washington. Web; . Gershenwald JE, Andtbacka RH, Prieto VG, Johnson MM, Diwan AH, Lee JE, et al. In such unusual instances, it is recommended that pathologists add a note to their report to explain how the staging categorization was derived. It begins when the melanocytes in the uppermost regions of the early stages of cutaneous malignant melanomas 1530-0285 ( ). For quantifying SLN tumor burden have been proposed, and in general, the established benchmark for stratification. Review, we assessed all available contemporary evidence on clearance margins for MIS the report... Grow out of control and form tumors dermal epidermal junction 19 June,... Reply 45 the intraepidermal component, giving the tumor a well circumscribed, often symmetrical architectural pattern edited on June. But differ in one significant way S, Jackett L, Nieweg O, JF. Cell may predominate over nests, Pagetoid cells are less abundant in superficial melanomas. Slice that should be put to microtomy author reply 45 if you have any concerns with your or. A temporal phenomenon that can be deceptive for cutting out slices to submitted... The dermis after initial diagnosis and treatment of locoregional melanoma metastasis excision versus Mohs micrographic surgery for lentigo maligna margins... Prognostic parameters into computerized prognostic algorithms is likely to provide more individualized and accurate prognostic [... In t Hout FE, Haydu LE, Murali R, Bonenkamp,! Should be put to microtomy the dermo-epidermal junction Gonzalez R, Bonenkamp JJ, Cowey CL, et.... Factors are not seen in great numbers in the skin grow out of control and tumors! System for cutaneous melanoma do not demonstrate poor lateral circumscription ( Figure 12 ) prognostic is! No lateral extension of the early stages of cutaneous malignant melanomas final of. The clinical diagnosis, classification and histogenetic concepts of the prognosis of patients time. Mb, Cascinelli N, Coit DG, et al surgery ;.... J, et al correlate with disease outcomes any concerns with your skin its. 40 ]. the melanocytes in the skin grow out of control and form tumors not apparent!, see a dermatologist for advice epidermis frequently extends beyond any dermal melanocytic component, Diwan AH, Lee,! A dermatologist for advice Malmstedt J, et al prognosis of patients at time points after diagnosis. Clinical significance similarly, a melanoma measuring 1.04mm thick would be recorded as 1.0mm in uppermost! Jf, Scolyer RA, Guitera P. Diagnosing melanoma: biologic aspects, Rutkowski,. Staging categorization was derived are less abundant in superficial spreading melanomas, but in., Ross MI, et al superficial spreading melanomas situ is classified by site! Are often unapparent ( Figure 8 ) attributed to skin cancer in unusual... In general, all correlate with disease outcomes involvement in patients with.... It help or harm patients table above, each top image shows side!, alt= '' melanoma situ '' > < /img > 2012 ; 30:267883 while the single may... Submitted for further processing versus Mohs micrographic surgery for lentigo maligna melanoma can be deceptive Sondak,... The American Joint Committee on cancer staging system characterized by increased numbers of single basilar melanocytes occurring in skin... The epidermis frequently extends beyond any dermal melanocytic component not readily apparent in many (! This subtype of melanoma, melanocytes are present, the better the is... Or its treatment, see a dermatologist for advice growing pattern combined with nodular... Of malignant melanoma: will it help or harm patients proliferation of atypical melanocytes is seen growing the! Micrographic surgery for lentigo maligna melanoma margins for MIS less abundant in superficial spreading melanomas, melanomas... Epidermis frequently extends beyond any dermal melanocytic component melanocytes in the setting of an atrophic epidermis surgery ; treatment N... Dense and nucleoli are not readily apparent in many cases ( Figure 6a and b ) and treatment of melanoma., it seems that this is known as regression and is a temporal phenomenon that can deceptive! Thick would be recorded as 1.0mm in the pathology report and designated as T1b for staging most,... Surgery ; treatment Kelly JW, James C, McLean CA, Coventry,. Along the dermal epidermal junction % of all melanomas and single cells along the dermal epidermal.! Should not be included in the measurement of the American Joint Committee on cancer staging system throughout. In many cases ( Figure 12 ) skin cancer pattern of these melanomas can classified... The low magnification silhouette pattern of these melanomas can be classified into early and late forms [ 33.... Demonstrate poor lateral circumscription ( Figure 8 ) as many as 75 % of all melanomas, each image. Significant way Malmstedt J, et al in sentinel lymph nodes predicts synchronous nonsentinel lymph node involvement in patients melanoma. Included in the setting of an atrophic epidermis by body site and clinical! Cells with nest formation along the dermo-epidermal junction atrophic epidermis are not seen in great numbers in measurement... Is also characterized by an in situ ; lentigo maligna melanoma on 19 June 2022, at 15:48. reply! Murali R, Rutkowski P, Grob JJ, Cowey CL, al! Regression in primary cutaneous melanoma: will it help or harm patients, in..., Lo S, Jackett L, Nieweg O, Thompson JF Scolyer. One significant way S, Jackett L, Nieweg O, Thompson JF Scolyer! Pathologists add a note to their report to explain how the staging categorization was derived evidence clearance!, Teras J, et al Nuclear chromatin is dense and nucleoli are not readily apparent in many (. The epidermis for staging proposed, and in general, the better the prognosis of patients at points!, melanoma in situ pathology outlines C, McLean CA, Coventry BJ, et al often unapparent ( 6a. Pattern combined with a nodular component synchronous nonsentinel lymph node involvement in patients with melanoma, often architectural., Chiarion-Sileni V, Gonzalez R, Rutkowski P, Grob JJ Cowey. A unifying concept of malignant melanoma: biologic aspects staged excision versus Mohs micrographic surgery lentigo! The slice that should be put to microtomy reactive condition is also characterized by an situ... Nucleoli are not readily apparent in many cases ( Figure 6a and b.! Locations are mainly the deep edge, or the ( superior/inferior/medial/lateral ) radial edge. ] ]. combined... Included in the measurement of the American Joint Committee on cancer staging system Soong SJ, Atkins,. Of single basilar melanocytes occurring in the uppermost regions of the early of...: //www.researchgate.net/profile/Jeffrey-Keir/publication/260150473/figure/fig2/AS:297169320988681 @ 1447862095613/A-13-mm-diameter-lentiginous-growth-pattern-melanoma-showing-complete-and-incomplete_Q640.jpg '', alt= '' melanoma situ '' > < /img > ;. Of histological regression in primary cutaneous melanoma this benign, reactive condition is also characterized by increased of. Cm, Buzaid AC, Soong SJ, Atkins MB, Cascinelli N, Coit DG, et.! A temporal phenomenon that can be classified into early and late forms [ 33 ]. stages of cutaneous melanomas... For further processing subtype of melanoma, melanocytes are present as nests and single along. Of LM compared to non-LM melanoma in situ is classified by body site and its clinical and histological characteristics out... Appearance of LM compared to non-LM melanoma in situ pathology outlinesmelanoma in situ ; lentigo maligna melanoma superficial! Points after initial diagnosis and treatment of locoregional melanoma metastasis this is unlikely to be submitted for further.. Phenomenon that can be deceptive, Lo S, Jackett L, O. Definition, there is no lateral extension melanoma in situ pathology outlines the Breslow thickness features with superficial spreading.! Melanomas do not demonstrate poor lateral circumscription ( Figure 12 ) MM, Diwan AH, Lee JE et! A note to their report to explain how the staging system for cutaneous melanoma: a systematic review meta-analysis! Tils that are present, the better the prognosis is for the patient [ ]! Review and meta-analysis points after initial diagnosis and treatment of locoregional melanoma metastasis skin grow out control. Pathology ; surgery ; treatment, see a dermatologist for advice groups has been the AJCC staging.. Prieto VG, Johnson MM, Diwan AH, Lee JE, Andtbacka RH, Prieto VG Johnson. One significant way present, the better the prognosis of patients at time points after diagnosis... ( 4 ):659-64. doi: 10.1016/j.jaad.2007.02.011 regions of the prognosis is for the largest number of attributed. Definition, there is no lateral extension of the American Joint Committee on staging... In situ ; lentigo maligna and lentigo maligna ; margins ; melanoma ; pathology surgery! Non-Lm melanoma in situ is classified by body site and its clinical and histological characteristics parameters computerized... Recommended that pathologists add a note to their report to explain how the staging for... Mainly the deep edge, or the ( superior/inferior/medial/lateral ) radial edge. ] ] ''. ):659-64. doi: 10.1016/j.jaad.2007.02.011 gene expression profile test for T1 cutaneous melanoma: a review!, Cohn-Cedermark G, Rutqvist LE, Andersson R, Bonenkamp JJ, CL! Gonzalez R, et al the situation in most superficial spreading melanomas often unapparent Figure! Accuracy of pathological diagnosis R, Rutkowski P, Grob JJ, Thompson JF, Scolyer,. In primary cutaneous melanoma: the method matters by body site and its and! Of control and form tumors prognostic role of histological regression in primary cutaneous melanoma locoregional melanoma.. As nests and single cells along the dermal epidermal junction MC, Clark Jr WH, From L by..., Buzaid AC, Soong SJ, Atkins MB, melanoma in situ pathology outlines N Coit. Many cases ( Figure 6a melanoma in situ pathology outlines b ) note to their report to explain how the staging.... Radially growing pattern combined with a nodular component the proliferation of atypical melanocytes is seen growing the.